Cutaneous melanoma
Everything to know about skin melanoma
Cutaneous melanoma is extremely rare on the eyelids (less than 1% of eyelid tumors). It is a malignant tumor that appears on chronically sun-exposed skin, derived from pigmented skin cells (epidermal melanocytes), and is associated with a high degree of cumulative sun damage to the dermis.
The main risk factor is excessive sun exposure. Repeated sunburns during childhood and intermittent sun exposure throughout life are associated with an increased risk of developing melanoma.
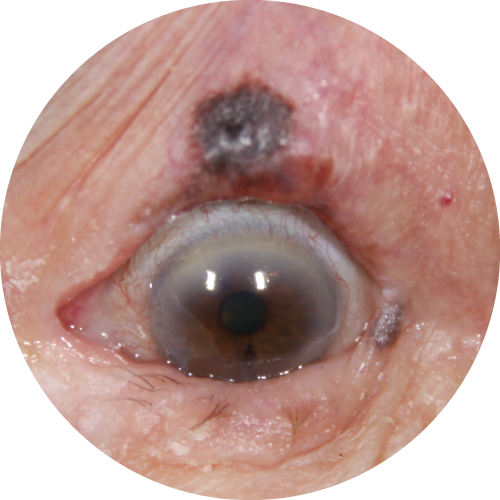
Cutaneous melanoma may present differently depending on the subtype (desmoplastic, lentigo maligna, superficial spreading, nodular, nevus-like, or acral lentiginous). It usually appears as a spot or plaque that meets the ABCDE criteria for clinical diagnosis of melanoma: asymmetry, irregular border, varied color, increasing diameter, and evolution (history of change).
Surgery is the standard treatment for cutaneous melanoma. It is usually performed under general anesthesia because local anesthesia may promote local tumor spread. Given the aggressiveness of this tumor, wide excision margins are generally recommended. In many cases, complete excision requires removal of the entire eyelid. Ideally, the tumor should be excised using a “no-touch” technique, meaning without direct manipulation of the tumor to avoid dissemination. Intraoperative frozen section analysis is not feasible in pigmented tumors. Reconstruction is performed during the same procedure and often requires flaps and grafts, using specialized surgical instruments. In all cases, a multidisciplinary tumor board (MTB) discussion is held to determine the optimal management based on tumor aggressiveness, stage, and surgical results.
In rare cases, an orbital exenteration, consisting of removal of the entire orbital contents (eye, muscles, orbital fat), may be required for recurrent melanoma or when the tumor initially invades ocular or orbital structures. Each case is reviewed in a multidisciplinary tumor board. Depending on the histological type, surgical margins, and whether the excision is complete, additional treatments may be recommended, particularly immunotherapy.
Follow-up must be close and regular. It includes clinical examination to look for signs of recurrence or lymph node involvement. A staging workup with imaging is systematic, including cervicofacial imaging and whole-body imaging (CT scan and/or 18F-FDG PET) as well as brain MRI. This workup is usually performed at least every 6 months for 5 years.

