Sebaceous Carcinoma
Learn everything about sebaceous carcinoma
Sebaceous carcinoma is a malignant epithelial tumor with sebaceous differentiation. It develops on the eyelids from the Meibomian glands, which are involved in the secretion of the lipid layer of the tear film. It is an aggressive and rapidly growing tumor with a risk of lymph node and visceral metastasis.
The main risk factors are excessive sun exposure, immunosuppression, certain oncogenic viruses (HPV), and Muir-Torre syndrome, although periocular sebaceous carcinomas have virtually no association with this syndrome.
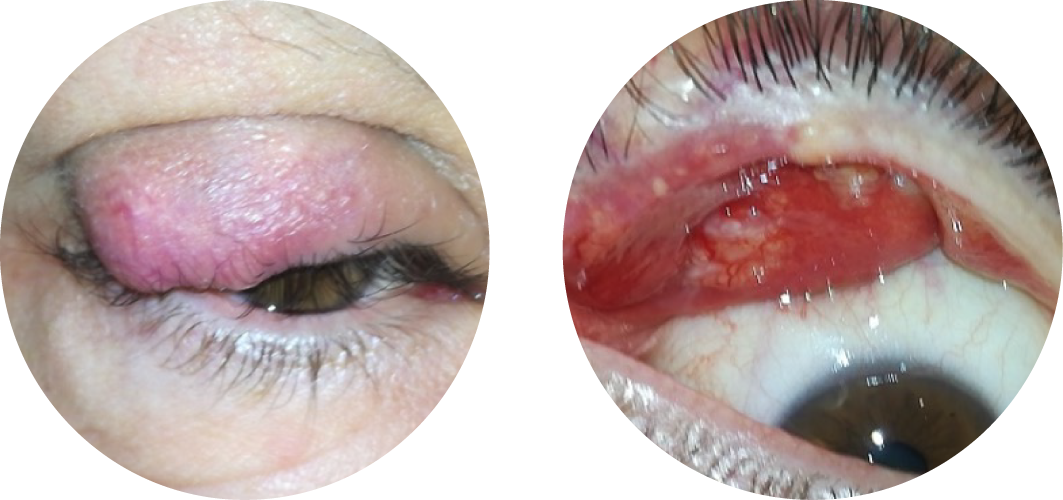
Sebaceous carcinoma usually occurs on the upper eyelid. Two main clinical presentations are described:
- Nodular form: presents as a firm, pinkish-yellow-brown lesion with rapid growth, often causing eyelash loss. This form can be mistaken for a chalazion, which is a common benign eyelid lesion.
- Pagetoid inflammatory form: presents as eyelid inflammation (chronic blepharoconjunctivitis or “carcinomatous blepharitis”), with poorly demarcated extension along the basal membrane of the conjunctival epithelium. Ocular surface inflammation with eye pain is frequently present.
In the presence of a persistent lesion in a patient over 50 years old, a biopsy under local anesthesia is usually recommended to rule out sebaceous carcinoma. However, the histopathological diagnosis can be challenging and may require review in a referral center or even a repeat biopsy.
Surgery is the reference treatment for eyelid sebaceous carcinoma. It may be performed under local or general anesthesia depending on the complexity and duration of the procedure. Given the aggressiveness of this tumor, wide resection margins are recommended to ensure complete removal. Reconstruction is performed during the same operation and often requires the use of flaps and grafts. An intraoperative histopathological assessment (“frozen section”) helps determine whether the tumor has been completely excised. In pagetoid forms, complete excision is not possible, requiring the use of adjuvant topical chemotherapy. In all cases, a multidisciplinary tumor board (MDTB) discussion is held to determine the optimal management strategy according to tumor aggressiveness, stage, and surgical outcomes.
In cases of incomplete excision, reoperation or radiotherapy may be considered. Radiotherapy (conventional external beam) may also be used in situations where surgery does not allow for complete excision.
Sebaceous carcinoma is an aggressive tumor with a risk of lymphatic metastasis. In addition to regular clinical follow-up, further staging with head and neck imaging (ultrasound, CT scan) and even whole-body imaging (18F-FDG PET scan) in cases of lymph node involvement should be performed during follow-up, after an initial preoperative staging evaluation to assess tumor dissemination.

