Basal cell carcinoma
Everything to know about basal cell carcinoma
Basal cell carcinoma (BCC) is a group of carcinomas that arise from the epithelial cells of the epidermis or from hair follicle stem cells. There are many morphological subtypes with distinct clinical and histological features, but with similar epidemiology and etiology. All types share the presence of nests of basaloid cells with hyperchromatic nuclei and minimal cytoplasm. On the eyelid, it is the most common tumor, accounting for about 95% of eyelid tumors. It is also the tumor with the best prognosis. Basal cell carcinoma demonstrates local aggressiveness but never metastasizes.
The main risk factors are excessive sun exposure and immunosuppression. In cases of multiple lesions in a young patient, a genetic origin (Gorlin syndrome, xeroderma pigmentosum) should be suspected.
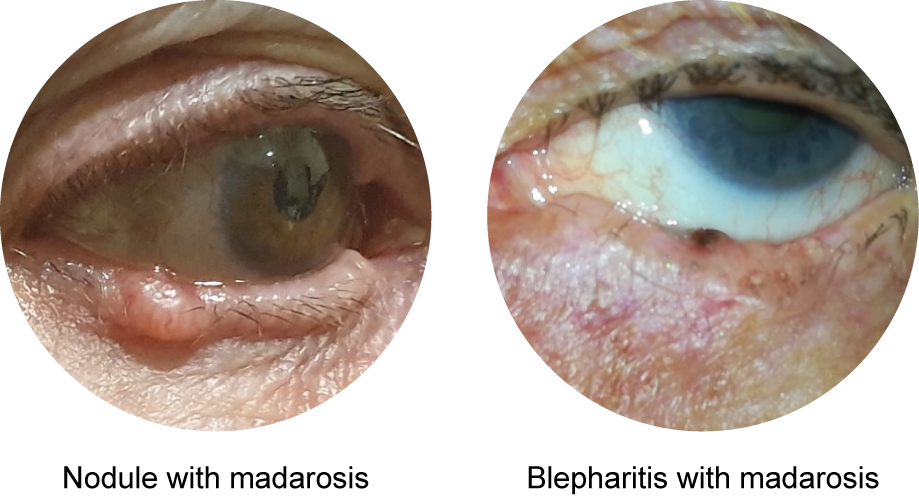
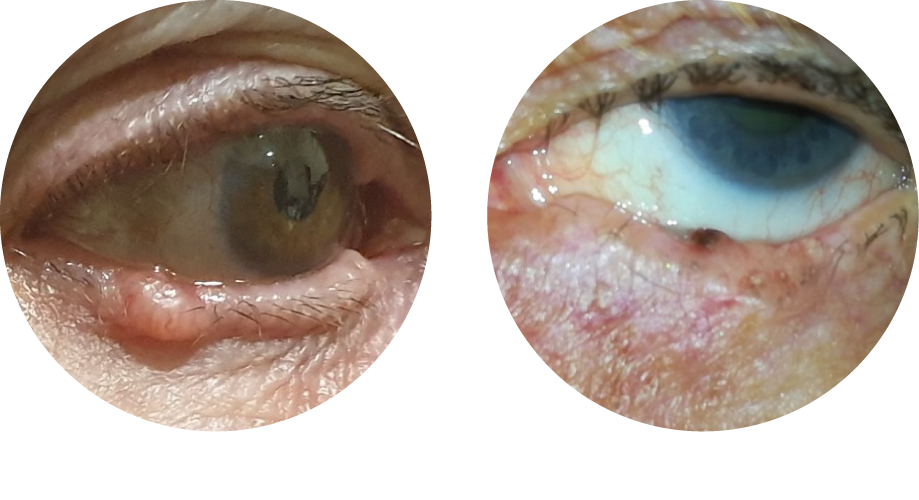
Basal cell carcinoma typically occurs on the lower eyelid. Clinically, it usually presents as a nodule with fine vessels on its surface. Ulceration, loss of eyelashes (madarosis), and bleeding when the lesion is scratched may also be observed. Sometimes, basal cell carcinoma may mimic chronic eyelid inflammation (blepharitis), which can lead to diagnostic pitfalls. Its growth is usually slow, over months to years. Occasionally, orbital imaging may be performed if intraorbital extension is suspected. A biopsy under local anesthesia in the clinic can confirm the diagnosis if there is uncertainty.
Surgery is the reference treatment for basal cell carcinoma. It allows complete tumor removal and reduces the risk of recurrence. Excision margins of 2 mm are generally sufficient, except for certain subtypes where wider margins are recommended.
Other treatments may be used, either in addition to or as an alternative to surgery. Radiotherapy (contact therapy or conventional external radiotherapy) may be considered in cases where surgery does not allow complete excision. Sonic Hedgehog pathway inhibitors (vismodegib and sonidegib) may also be used for locally advanced basal cell carcinoma, orbital invasion, or in cases of multiple tumors (Gorlin syndrome). They often achieve tumor regression, although at the cost of numerous side effects.
Follow-up is generally clinical and performed every six months. An annual dermatologic follow-up is recommended since other tumors may appear on the face.