Conjunctival Melanoma
Everything you need to know about conjunctival melanoma
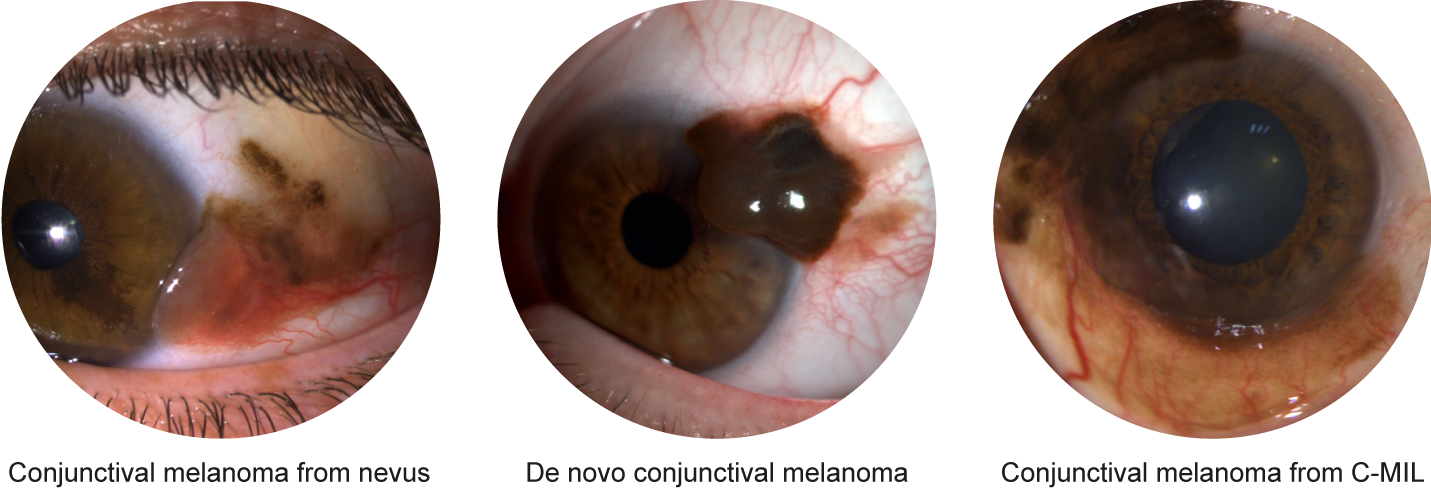
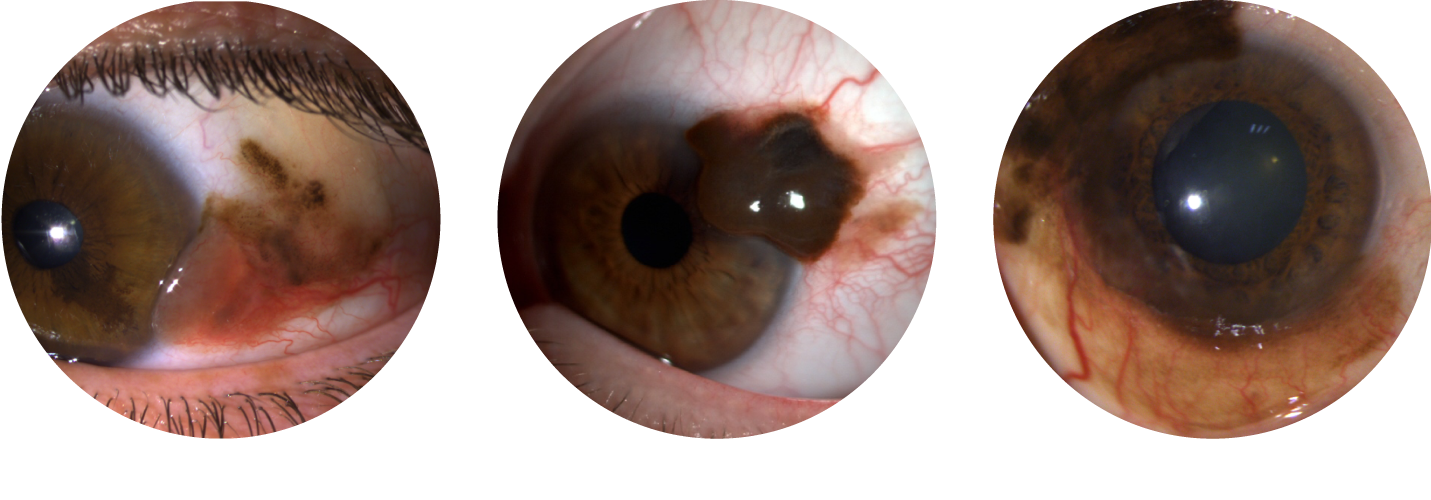
Conjunctival melanoma is a malignant tumor of the conjunctiva that develops from pigmented cells called melanocytes. These cells are naturally present on a structure called the basal membrane, or they can be distributed on both sides of the basal membrane in the case of a conjunctival nevus ("mole"). When they transform into cancerous cells, their proliferation can:
- remain confined to the basal membrane: referred to as a conjunctival melanocytic intraepithelial lesion (C-MIL)
- involve both the epithelium and the stroma, on both sides of the basal membrane: referred to as an invasive conjunctival melanoma


Although precise statistics are not available in France, the incidence of malignant conjunctival melanocytic tumors is low. Conjunctival melanoma accounts for 5% of all ocular melanomas and is the second most common malignant tumor of the conjunctiva after epithelial malignancies. It is a rare tumor.
Like malignant epithelial tumors, sun exposure appears to be the main risk factor for the development of conjunctival melanoma or C-MIL. However, the exact mechanisms remain unclear, as some conjunctival melanomas can develop in areas protected from light (under the eyelid).
Malignant conjunctival melanocytic lesions are generally pigmented, although some may not be. It is not possible to precisely identify these tumors without analysis. Depending on their origin (C-MIL, nevus, or de novo), these lesions may present as flat or nodular pigmented lesions, requiring prompt evaluation by an ocular oncology specialist.
The first step of treatment involves surgical excision to determine the exact tumor type. Surgery should always be performed in a specialized center, as local recurrences are more frequent when initial surgery is done elsewhere. Complete excision may not always be possible, requiring limited surgery. Adjuvant treatment is generally necessary, via topical chemotherapy (for C-MIL) and/or radiotherapy (for invasive conjunctival melanoma).
Ophthalmologic follow-up will be specified by the referring ocular oncologist and should be long-term since local recurrences are possible, even after 5 years from initial treatment.
Systemically, the presence of stromal infiltration (invasive melanoma) makes the development of metastases possible. These may appear in conjunctival drainage territories (lymphatic spread), including the facial and cervical lymph nodes, or distant organs such as the lungs, liver, or bones (hematogenous spread). Imaging of the cervical region on the same side as the affected eye, as well as whole-body imaging for 5 years, is essential to detect early lymph node or distant metastases, which may require specific treatment (surgery ± radiotherapy, targeted therapies, or immunotherapy). The overall metastatic risk remains low but is higher than for malignant conjunctival epithelial tumors and depends on the initial tumor stage.

