Conjunctival Carcinoma
Everything to know about conjunctival carcinoma
Conjunctival carcinoma is a malignant conjunctival tumor that develops from cells of the conjunctival epithelium. These cells are naturally present on a structure called the basal membrane and can accumulate abnormalities over time. Initially, when they transform into cancer cells, their proliferation will remain limited to the epithelium: this stage is called conjunctival epithelial dysplasia up to the conjunctival carcinoma in situ stage.


Subsequently, this proliferation may cross the basal membrane to reach the stroma, allowing cells to migrate outside the conjunctiva (potentially causing metastases): this stage is called invasive conjunctival squamous cell carcinoma. Some tumor cells may also evolve into a more aggressive form, known as invasive conjunctival adenosquamous carcinoma.


Chronic exposure to ultraviolet (UV) B radiation is the most important environmental causal factor in the development of malignant epithelial tumors. By locally suppressing cell-mediated immunity, UVB also enhances other risk factors such as immunosuppression (due to HIV infection or immunosuppressive treatment after organ transplantation) or the effect of oncogenic viruses such as human papillomavirus (HPV).
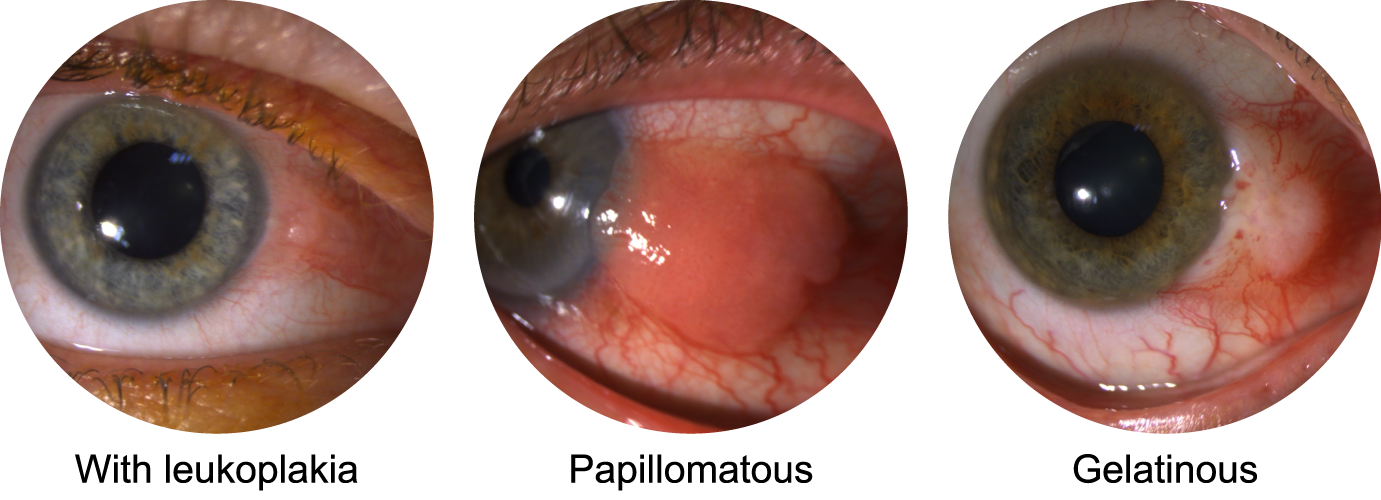
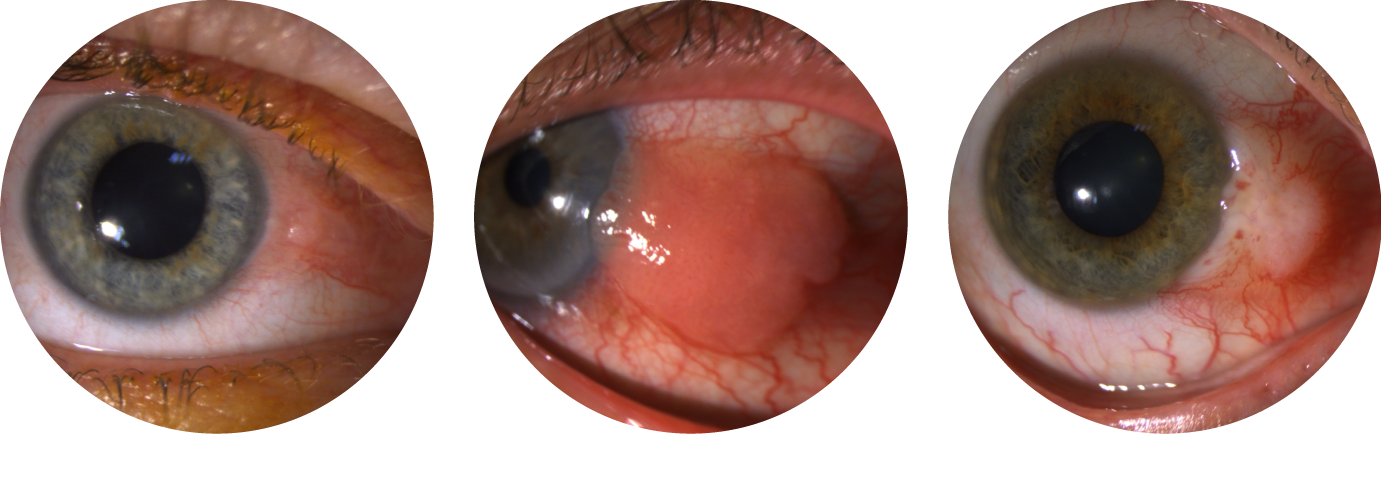
Malignant conjunctival tumors share common clinical features, which is why histological analysis after excision is important for differentiation. Overall, their appearance is variable:
- gelatinous, flat and translucent (very common in corneal involvement) or raised
- papillomatous, slightly or strongly raised
- leukoplakic with a surface keratin plaque
The first step in treatment involves surgical excision to determine the precise tumor type. However, even if clear margins are obtained, adjuvant treatment is usually required.
In cases of severe dysplasia or carcinoma in situ, topical chemotherapy is typically proposed.
In more advanced cases (invasive squamous cell carcinoma or invasive adenosquamous carcinoma), radiotherapy is necessary to reduce the risk of local recurrence.
Ophthalmologic follow-up will be determined by the referring ocular oncologist, but it must be long-term because local recurrences are possible even after 5 years from initial treatment.
Systemically, the presence of stromal infiltration (invasive squamous or adenosquamous carcinoma) may lead to metastases. These can occur in the conjunctival lymphatic drainage areas, namely the facial and cervical lymph nodes. Cervicofacial imaging (usually ultrasound) on the same side as the affected eye is essential for 5 years to quickly detect nodal metastases, which will require specific treatment (surgery ± radiotherapy). Overall, the risk of metastasis is low but depends on the tumor's initial stage.

